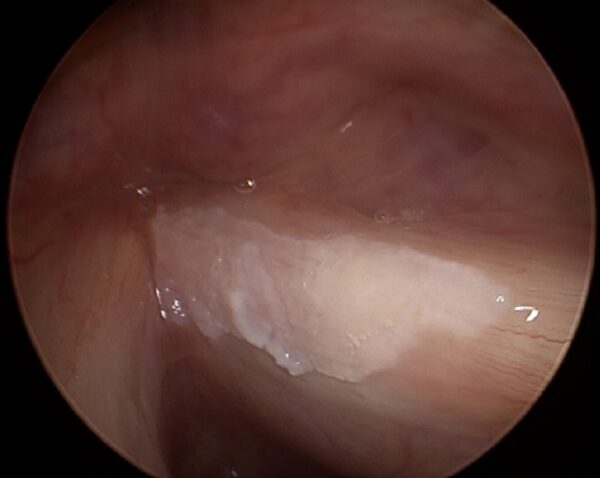
Leukoplakia may be a precursor or an early sign of malignant change (e.g., laryngeal cancer). Leukoplakia is often reflexively equated with the presence of dysplasia, which must be histologically clarified or at least closely monitored.
In addition to dysplasia, the differential diagnosis of leukoplakia may include biofilm formation, fungal infection, or superficial scarring. White deposits may also occur after using asthma sprays containing cortisone (SIL: Steroid Inhaled Laryngitis).
Only a histological examination of the tissue can provide information as to whether the leukoplakia is a symptom of incipient laryngeal cancer or whether it is merely a benign change in the tissue structure.The surgical removal of a leukoplakia does not primarily improve the voice; on the contrary, it can even worsen it. There are two opposing goals in such an operation: On the one hand, one would like to remove everything or take a representative sample with as much certainty as possible. The exclusion or removal of malignant changes has priority. On the other hand, one would like to avoid, as far as possible, a serious deterioration of the voice due to scarring or substance deficits. With experience and consideration of the endoscopic and stroboscopic findings, both goals can often be achieved.
Leukoplakia may recur after surgical removal. Especially in these cases, a new and helpful alternative to repeated surgical ablation is photoangiolytic laser treatment with the KTP laser or the Blue laser.