Recurrent nerve paresis – what is it?
affected and the other side remains intact.
About 10,000 times a year in Germany, the diagnosis „Recurrent paralysis“ is provided. A proven method to treat the consequences of unilateral recurrent paralysis is vocal fold augmentation. The further development of implants and surgical techniques opened up new possibilities. Recurrent nerve paralysis is damage to the laryngeal nerves (recurrent nerves) and leads to laryngeal palsy. As a result, the movement of the vocal cord of the affected side is disturbed. As a result, the vocal sound is breathed, quiet and hoarse. In some patients, only the loud voice is affected. Often there is also a swallowing disorder. All of these symptoms of unilateral recurrent paralysis can usually be treated well with an „augmentation“ of the paralyzed vocal cord.
Listen to David before and after his vocal fold augmentation
Recurrent paresis (also called vocal fold paralysis, laryngeal paralysis, paresis, vocal fold arrest, vocal fold reduced mobility) is damage to the laryngeal nerve (recurrent nerve) and leads to paralysis of the vocal fold. Causes of vocal cord paralysis are often operations or diseases of the neck or upper thorax (i.e. thyroid, carotid artery, cervical spine, heart, lungs, lymph node enlargement but also metastases). Often, however, there is no identifiable cause. As a result, the movement of the vocal fold of the affected side is disturbed, and the vocal folds no longer close properly.
Our voice clinic is highly specialized in diagnosing all reasons and effects of Recurrent nerve paresis and offers state-of-art therapeutical options to regain a mostly normal voice function. Patients from all over the world visit us for phonosurgical treatment.
Augmentation
A well-known method for more than 100 years is the so-called vocal fold relining or vocal fold augmentation, in which a substance is introduced into the area at the side of the vocal fold and the vocal cord is thereby displaced to the middle.
This can be done in local anesthesia (through the mouth or the skin from the outside) or under general anesthesia. There are many different substances available, which differ mainly in terms of their consistency, strength, and absorbability over time. Frequently used substances are i.a. Hyaluronic acid, and endogenous fat. We use all preparations as well as the body’s fat and have experience with all implants available on the market. If a paresis has appeared fresh and to hope for spontaneous recovery, first quickly resorbable substances come into question (resolution selectable within weeks to months). A vocal fold augmentation can then also be considered as a „trial injection“ with a resorbable substance. If the paresis has existed for some time or if it is known that the nerve has been permanently damaged – for example, if, according to the surgeon, it had to be resected during a tumor operation („sacrificed“), then u.U. equal to a permanently effective surgerz will be performed.
In most cases, this operation is possible on an outpatient basis. We have not seen any serious complications after more than 600 outpatient augmentations.
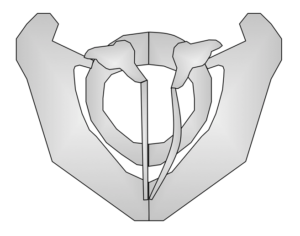
Immobile Vocal Fold