
Gender-affirming voice and communication change
Sounds really feminine!
If a person’s voice doesn’t match their gender, you don’t have to accept it; you can do something about it. If you feel you belong to the female gender, you want to be perceived as such and addressed as such, for example on the phone. Every time! When the voice does not match the identity, it often leads to frustration, silence or social isolation. We want to help women develop a voice and appropriate communication that reflects their true gender. Voice feminisation is an important step in the overall process.
Anna about her voice feminization surgery
Voice examples before and after voice feminization surgery
A lot more voice examples you’ll find on our YouTube-Chanel
A patient from Norway shares her VFS experience with Prof. Hess on reddit
At the MEDICAL VOICE CENTER we offer a team approach. Our SLPs offer gender affirming voice training in resonance, speech patterns, efficient voicing, and pitch, while our laryngologist offers pitch-raising surgery through modified Wendler glottoplasty. Throughout the process, we work closely with the patient to meet their individual goals and empower them to make informed decisions.
The goal is a voice that, in the overall context of speaking, has all the feminine characteristics that make up a woman’s voice. Vocal enhancement surgery alone is unlikely to provide completely satisfactory results.
The MEDICAL VOICE CENTER is a renowned voice centre specialising in voice feminisation surgery. We take our time with each patient, listening carefully and not letting go until we have understood all your concerns and sensitivities.
Prof. Hess is the president of the International Association of TransVoice Surgeons.
A very experienced surgeon
Markus M. Hess, MD, PhD, routinely performs voice raising procedures, a total of approximately 60-80 glottoplasties per year. He lectures worldwide and is a leading researcher in the field of surgical techniques and Trans*Voice Therapy. The voice therapy developed by Prof Hess in collaboration with leading SLPs is specifically tailored to the needs of trans patients.
Voice feminization surgery focuses on raising the pitch and reducing the ability to produce a deep voice. The goal is a voice that has all the qualities of a female voice. To achieve this, the new voice needs to be trained by a professional voice therapist after surgery. The integration of gender affirming voice training and surgery is essential to improve the outcome of the treatment.
The MEDICAL VOICE CENTER has developed a special post-operative voice feminization therapy for women who wish to have an authentic female voice and match their gender identity. This gender affirming voice training is part of our feminisation package.
Prof. Markus M. Hess explaining voice feminization surgery (Glottoplasty) and the post-operative behavior.
„For me, a female voice means no longer being tense. Being able to let go! I was always just tense. Physically as well as mentally. The voice is the residue of tension that I still feel from my previous life. And I want to get rid of that tension too.“
K.J. April 2021
The most common surgical techniques for voice feminization are described here (in German language)
Preparing your voice feminization surgery
The voice change process starts with a detailed interdisciplinary initial discussion together with the surgeon as well as the speech therapist (voice and speech trainer). This interview will also analyze the potential need for post-operative vocal therapy. Our treatment package ‚voice-feminization’ comprises interdisciplinary history taking with a physician (ENT doctor) trained in voice disorders / phonosurgery and a speech language pathologist specially trained in clinical voice disorders / vocal coaching. Diagnostics include videostroboscopy, endoscopy, electroglottography, electroacoustic voice analyses, perceptual voice assessment, voice range profile, Acoustic Voice Quality Index, Trans Women Voice Questionnaire, and further tests. Subsequently, a detailed briefing and discussion are offered. In case of surgery, a consent form is handed out explaining in detail all options for the following voice feminization procedure.
Prof. Markus Hess provides you with information about treatment options and alternatives (conservative and surgical) and explains to you all possible surgical procedures.
Glottoplasty costs
The expertise of the surgeon makes a big difference.
Microsurgical voice feminization is a routine procedure for very few surgeons. Personal knowledge, operative experience with exactly these issues of glottoplasty, technical microsurgical adeptness as well as the constant operation routine and frequency are the decisive factors for the success of the operation.
Absolute specialists are often more expensive than generalists who perform the procedure only occasionally to expand their portfolio. When choosing a surgeon, be guided by the surgeon’s specialist expertise and success rate – not by prices. You should choose wisely who you trust with your voice.
The voice feminization surgery
The voice feminization surgery (glottoplasty) are based on three keystones:
– Shortening of the vocal cords.
– Change the vibration dynamics of the vocal cords.
– Reduction of the vibratory mass of the vocal cords.
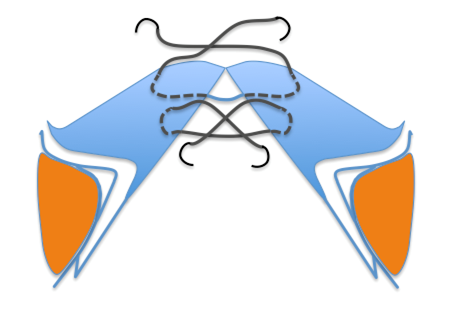
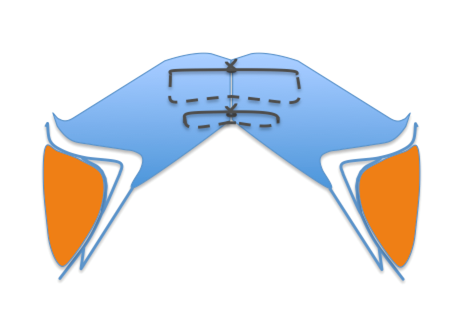
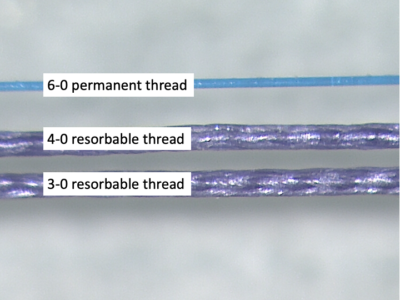
Outpatient glottoplasty is painless and under general anaesthesia. The only a few millimeters short vocal cords are permanently connected with two hair-thin, firm threads.
This surgery creates a web at the front of the V of the vocal cords. This shortens the vocal cords to help raise voice pitch. Anterior glottal web formation affects frequency range by eliminating the ability to produce lower pitch.
An additional injection of the vocal folds with a temporary implant reduces the tensile forces on the sutures during the postoperative period. Depending on the vocal fold volume, ablation will be perform using the LAVA method. In addition, if necessary, the vocal folds are temporarily sedated with Botox.
Setting the sutures in a voice-feminization-surgery (glottoplasty)
Voice feminization surgery and aftercare
The surgery will be carried out by Prof Hess on an outpatient basis. The operation takes place in the Ambulatory Surgery Centre (AOZ), which is about 200 metres away. There we work with very experienced and highly qualified medical staff. After the surgery under general anaesthetic, you will be monitored in the recovery room. Approximately 2 hours later, you will be seen at the MEDICAL VOICE CENTER for a post-operative video laryngoscopy and a detailed after-care consultation and discussion of the next steps. As a general requirement in Germany, all patients undergoing general anaesthesia must be accompanied for 24 hours.
The next day you will be seen for a check-up and further appointments will be made. We will discuss your follow-up appointments for the next few months.
Your therapeutic care will include pre- and/or post-operative speech training according to your personal needs. We offer you 6 sessions, which can be scheduled individually and/or in conjunction with your medical follow-up. Post-operatively, the first hour of voice training takes place after the voice has been „released“ by Prof. Hess. Therapy via Skype/Teams is possible at any time.
Medical follow-up
We individually discuss the follow-up examinations in the following months. Usally after 2 and 6 weeks and 6 and 12 months for laryngeal examinations, acoustic analysis, and new voice recording.
Your therapeutical care includes pre-and / or postoperative speech training or speech therapy according to personal needs. We offer 6 sessions, individually planable also in double lessons, in blocks, and/or in connection with the medical follow-up. Postoperatively, according to our rehabilitation scheme, it will soon be possible to whisper ‚loose‘ again.
Targets of gender affirming voice training (Trans*Voice Therapie)
Prosody:
Prosody is the melody of speech and includes changes in loudness, pitch and stress. Men tend to use stress or loudness for emphasis, while women often use higher pitch variability.
Vocal resonance:
This term often refers to the perception of vibrations when using the voice. The location of vocal resonance isn’t entirely dependent on your gender. You may have a throat resonance, where the vibrations are concentrated in the throat or chest, or a frontal resonance, where the vibrations are felt around the lips and nose. A speech and language therapist can help you find a healthy resonance that reflects who you are. This requires practice, exploration and experimentation with your voice.
Therapy will also address
– Voice quality
– Articulation
– Speech rate and phrasing
Non-verbal communication such as eye contact, use of hand gestures, facial expressions, posture and head nodding.
The voice feminization package contains:
– Pre-operative voice training – Post-operative voice rehabilitation – Sociocultural feminisation – Surgery (glottoplasty) and medical follow-up – gender affirming voice training (articulation, intonation and resonance) – Resilience training for the new voice – Reinforcement of female pitch and resonance – Coaching and conversations on authentic female communication patterns.
Your therapeutic care includes post-operative speech training or speech therapy according to your personal needs. We offer you 6 sessions, which can be individually planned in double lessons, in blocks and/or in connection with the medical follow-up. Post-operatively, you will be able to whisper ‚loosely‘ immediately following our rehabilitation programme.
Our package includes a full range of medical and non-medical services, where multidisciplinary voice care and consultation are mandatory and always well received.
Modern, cosmopolitan and highly professional
In the MEDICAL VOICE CENTER, the diagnostic and therapy areas are physically separated from the state-of-the-art operating theatre. When you first enter the MEDICAL VOICE CENTER, the bright, modern feel-good atmosphere and the interior design with its design elements create a welcoming and cheerful ambience that does not remind you of a clinic. This is where preliminary discussions, examinations, aftercare and voice therapy take place. We offer a safe, trans-affirming environment. The surgery itself takes place in the Ambulatory Operation Centre (AOZ), which is about 200 metres away and is equipped with the latest technology.

FAQ – Frequently Asked Questions
This question is one of the most important and encompasses every point that is changing after surgery. Because voice is such a complex entity, we always have to find out what the individual’s expectations are – ranging from easily measurable F0 to personal favorable timbres and self perception. The expectations are not easily reduced to items in a questionnaire – that is why we thouroughly have to go through the individual’s history and (voicing) capabilities. That having said, we always try to find out if realistic expectations can be found. Otherwise, the indication for surgery should be thought over, or surgery should be cancelled.
Glottoplasty is one of the safest methods to raise the pitch, if the vocal folds can be accessed via direct microlaryngoscopy (which is frequently possible). However, the way of webbing and suturing can always lead to postoperative hoarseness and therefore this point has to be pointed out in the preoperative informed consent.
If the vocal folds have already been pretreated, then they can no longer vibrate symmetrically after a second intervention. That’s why good (first) surgery is so important. Improper surgery can cause hoarseness. However, there could be temporary complications such as pitch instability, foreign body sensation in the throat, rough voice – but these symptoms are all temporary.
Although we would be very happy to predict surgical outcome, each individual’s anatomy, physiology and voice technique and are so variable that we cannot predict the outcome. Still, our evidence comes from experience and systematic analysis. I do believe that – with time – we will come up with more reliable preoperative assessments that may predict better what will result from interventions of any kind. That’s why science is very helpful in medicine including voice therapy and vocal coaching.
After glotoplasty, the modulatory ability is preserved because the vocal fold tensioner (the so-called CT muscle) is not touched.
The witing time depends on the availability of our logopedist and surgery, because we always combine both interventions. Within the last months we receive many requests, so that we allot more time and space. The waiting time is roughly 6-8 weeks.
In the MEDICAL VOICE CENTER we recommend an adequate mechanical stimulation of the vocal folds in the early healing phase, since, according to recent research, this leads to better functional results. In other words – direct postoperative whispering is allowed. The voiceless whispering is trained before surgery. The women need to communicate, otherwise they stay in isolation.
By definition, whispering is a kind of unvoiced speech in which the speech sounds are not formed with the vocal folds. It’s a noise, not a sound.
Absolute vocal silence we consider only limited and maximum for three to five days. As a rule, our patients are allowed to whisper in a low voice.
The recommendation to be silent for several weeks or month after a voice feminization surgery and not to whisper is widespread. Many colleagues feel safe with this recommendation, because the total vocal rest is difficult to verify. Thus, possible, unsatisfactory results, always be justified by a non-observed speech prohibition.
Yes, you can. But it narrows the airway to some degree. As a result, this surgery (glottoplasyty) might be less appropriate for highly singing professionals (opera) and, perhaps, serious athletes.
No, we reject this in the MEDICAL VOICE CENTER. A sole voice feminization surgery in very few cases leads to a completely satisfactory result.
The Trans*Voice speech therapy can be done but without feminization surgery. It is important to know that working on the voice can be very hard. You must practice out of your comfort zone and consistently. There can be setbacks in the process that can cause frustration and disappointment. THAT IS NORMAL. However, if you are ready and motivated to hold on to strenuous vocal exercises, then the first step is already done.
With a voice feminization operation, we can significantly facilitate and shorten individual areas in the therapy process. First successes are likely to come faster, but even here, setbacks are possible and you will not be spared continuous training.
Clearly: coughing, to clear one’s throat, sneezing and loud screaming. The techniques, to avoid these are trained by our speech therapist before the surgery.
Only after a healing phase, which can last at least 14 days, if not a few weeks, a voice feminization is achieved.
Experience has shown that there is a slight, temporary swelling of the tissue immediately after the operation, so that the voice that can be heard directly after the operation will not already be the permanent state. In general it takes 6 – 12 month to achieve a truly feminine voice.
Yes, that’s the best. The day before and the day after the surgery, please come again for a follow-up examination and further concrete scheduling. We discuss the follow-up examinations in the following months (according to individual agreement).
After a glottoplasty everything can be eaten and drunk. Avoid the consumption of very spicy foods; Dairy products, nuts and red wine promote the formation of slime. In addition, there is a risk of reflux in case of wrong nutrition. Observe yourself what is (not) good for you, everyone reacts differently.
Drink sufficient, preferably (still) water, which ensures well-moistened mucous membranes.
Pitch is determined by the combination of length, mass and tension. You may look up the physics formula online. To whatever extent as surgery can change these parameters, the comfortable speaking pitch will be changed.
- Shorter cords lead to a higher pitch.
- Tighter cords lead to a higher pitch.
- Thinner vocal cords lead to a higher pitch.
It is the same as a string on a guitar.
After a glottoplasty you should do without sports for about 6 weeks. Caution with weight training:
To stabilize, the body uses the vocal fold closure. Pressing exercises (for example strength training, heavy lifting but also intercepting movements, for example in balance exercises) can endanger wound.
If you can present a medical certificate certifying that you can not be operated on due to a physical condition, the operation will be postponed for free.
No, unfortunately you can not. We only accept bank transfers or cash payments.
A dehydration of the laryngeal mucous membranes by the narrowed glottis does not occur. The exhaled air has 100% humidity. Much more, normal nasal breathing plays a role with its three functions of dirt filtration, heating and humidification.
Glottoplasty and swallowing: none of my patients that ai recall reported of swallowing problems in terms of aspiration (fluids or solid food goes into the trachea). Postoperative discomfort and rarely pain in the first days after surgery result from the laryngoscope placed into the larynx. But this is not related to the webbing and therefore not the cause.
Deep breathing: In terms of deep breathing, all patients are able to inhale and exhale the same air volume as before. In terms of rapid (maximum) flow there surely is a limitation after both procedures. Fortunately, airflow is (physiologically) mainly directed in the posterior larynx and even behind the vocal processes. However, if maximum and high effort breathing is an extremely important part of life, both surgeries should not be performed. But in the vast majority of our patients this is not the case.
Loud screaming: There is a restriction for loudest voice after glottoplasty.
James Thomas:
Dr. Kim is an outstanding surgeon. However, I don’t believe the tools make the surgeon. The surgeon should use a scalpel or a laser based on their comfort with the tool. If I were a patient, I would not make a decision based on the tool that the surgeon uses. The idea of making the web connect lower along the anterior margin so the air flows more smoothly is an interesting theory. In the individuals I have examined, I haven’t seen any difference in the subglottic area between different surgeons, including Dr. Kim’s patients.
Markus Hess
In our daily phonosurgical practice patients very often ask for ‘laser’ surgery, as if the laser was ‘magic’. The laser is an instrument and only as good as the hands controlling it. Although lasers are very important for phonosurgery, I must say that the patient should rather ask for the best technique and equiment that is on the market for a specific task and then ask if the surgeon has experience with this best technique – including the question if the surgeon has the specific tools. In highly specialised centers these tools will be available. So, in essence, surgeons think different to achieve best results: they choose from a spectrum of different instruments within their armamentarium, and if lasers work better for them than ‘cold steel instruments’, then its fine – and probably the best choice for their patient as well.
The concept and hope, that less turbulence due to ramping the air flow at the anterior subglottic site would result in clearer voice outcome, is compelling. If this concept were adequate and correct, it would make sense to put a lot of effort into this surgical step of the glottoplasty procedure. From our own experiences and from subglottic laryngoscopies in postoperative patients who had glottoplasties performed from other surgeons we could not see big differences, if any, from their subglottic anatomy that would prove that this funnel effect is actually achieved, and this also includes patients that I saw who were operated by Dr. Kim. At any rate, aerodynamics of phonation are very complex and there is at this stage of scientific research no method that can prove of disprove this concept.
When comparing these two surgical approaches, one must bare in mind that all individuals have – more or less – different voice boxes (laryx anatomy varies a lot interindividually). The angulation of the thyroid cartilages and the lengths of vocal folds as well as their thick are very different. It is like the shape and consistency of our faces, noses, ears etc.. Therefore, a technically exactly similar performed surgery can turn into a great result in one female and in others there might be only favourable results.
If one wants to start with a less invasive surgery, it seems clear that surgery only addressing the length and shape of vocal folds is less invasive and risky than doing an open neck surgery. Most females decide to have a glottoplasty and preserving the laryngeal framework anatomy and supplement with phonatory and voice therapy as well as vocal coaching for improvement of voice feminization.
However, a comparison of these two methods is not ‘fair’ in terms of what these technique aim for: FemLar attempts resonance changes as well as fundamental frequency (F0) changes and adds the Adam’s apple reduction, whereas glottoplasty and vocal fold shortening and retrodisplacement of the anterior commissure (VFSRAC) does not.
In general, singing styles differ significantly (classic to non-classic, hobby to high professional). And even for a surgically untreated larynx professionality in singing is still in most cases an enormous challenge. The more the singing is relying on a perfect, clear voicing and soprano-like easy onset in highest pitches, one might not go for any feminization surgery risk. One of the challenges is that the vocal fold mass, tension, length and tissue characteristics not only change with surgery, but also change with hormones and voice use. Too many variables to reliably predict outcome yet. But many researchers are working on this, including us.
If singing is the main priority or income in life, then avoiding any surgery may be the optimum option.